Barbara Johnson, BSN, RN, CPC, FHFMA Senior Revenue Cycle Consultant
Under HIPAA, all payers, including Medicare, are required to use claims adjustment reason codes (CARCs) and remittance advice remark codes (RARCs) approved by X12 recognized code set maintainers, instead of proprietary codes to explain any adjustment in the claim payment. RARCs are used to provide additional explanation for an adjustment already described by a CARC or to convey information about remittance processing. The following RARCs related to the No Surprises Act have been approved by the RARC Committee and were effective as of March 1, 2022.
The No Surprises Act provisions that apply to the claim
RARC #
RARC Text
N864
Alert: This claim is subject to the No Surprises Act provisions that apply to emergency services.
N865
Alert: This claim is subject to the No Surprises Act provisions that apply to nonemergency services furnished by nonparticipating providers during a patient visit to a participating facility.
N866
Alert: This claim is subject to the No surprises Act provision that apply to services furnished by nonparticipating providers of air ambulance services.
How cost sharing was calculated under the No Surprises Act
RARC #
RARC Text
N862
Alert: Member cost share is in compliance with the No Surprises Act and is calculated using the lesser of the QPA or billed charge.
N867
Alert: Cost sharing was calculated based on a specified state law, in accordance with the No Surprises Act.
N868
Alert: Cost sharing was calculated based on an All-Payer Model Agreement, in accordance with the No Surprises Act.
N869
Alert: Cost sharing was calculated based on the qualifying payment amount, in accordance with the No Surprises Act.
N870
Alert: In accordance with the No Surprises Act, cost sharing was based on the billed amount because the billed amount was lower than the qualifying payment amount.
Initial payment amount
RARC #
RARC Text
N871
Alert: This initial payment was calculated based on a specified state law, in accordance with the No Surprises Act.
N877
Alert: This initial payment is provided in accordance with the No Surprises Act. The provider or facility may initiate open negotiation if they desire to negotiate a higher out-of-network rate.
Final payment amount
RARC #
RARC Text
N863
Alert: This claim is subject to the No Surprises Act (NSA). The amount paid is the final out-of-network rate and was calculated based on an All-Payer Model Agreement, in accordance with the NSA.
N872
Alert: This final payment was calculated based on a specified state law, in accordance with the No Surprises Act.
N873
Alert: This final payment was calculated on an All-Payer Model Agreement, in accordance with the No Surprises Act.
N874
Alert: This final payment was determined through open negotiation, in accordance with the No Surprises Act.
Denial of Payment
RARC #
RARC Text
N876
Alert: This item or service is covered under the plan. This is a notice of denial of payment provided in accordance with the No Surprises Act. The provider or facility may initiate open negotiation if they desire to negotiate a higher out-of-network rate than the amount paid by the patient in cost sharing.
Notice and Consent
RARC #
RARC Text
N878
Alert: The provider or facility specified that notice was provided and consent to balance bill obtained but notice and consent was not provided and obtained in a manner consistent with applicable Federal law. Thus, cost sharing and the total amount paid have been calculated based on the requirements under the No Surprises Act, and balance billing is prohibited.
N879
Alert: The notice and consent to balance bill, and to be charged out-of-network cost sharing, that was obtained from the patient with regard to the billed services, is not permitted for these services. Thus, cost sharing and the total amount paid have been calculated based on the requirements under the No Surprises Act, and balance billing is prohibited.
Miscellaneous
RARC #
RARC Text
N830
Alert: The charge[s] for this service was processed in accordance with Federal/ State, Balance Billing/ No Surprise Billing regulations. As such, any amount identified with OA, CO, or PI cannot be collected from the member and may be considered provider liability or be billable to a subsequent payer. Any amount the provider collected over the identified PR amount must be refunded to the patient within applicable Federal/State timeframes. Payment amounts are eligible for dispute pursuant to any Federal/State documented appeal/grievance process(es).
N859
Alert: The Federal No Surprise Billing Act was applied to the processing of this claim. Payment amounts are eligible for dispute pursuant to any Federal documented appeal/ grievance/ dispute resolution process(es).
ParaRev can help
With almost 90% of consumers being surprised by either an unexpected medical bill or a bill that was more than expected1, it’s important to understand and use the appropriate RARC Codes Related to the No Surprises Act.
Hospital resources are finite, and with the constantly evolving environment of healthcare, codes and billing requirements can be hard to manage. Under the ParaRev Coding and Compliance Department, the Data team serves as a relief valve to ensure that the changes we are proposing our implemented in a timely and accurate fashion.
With coding and billing requirements constantly changing, many organizations are overwhelmed with maintaining billing systems and find annual pricing updates also a challenge. ParaRev has the capability to assist the hospital in the implementation of updated CPT®/HCPCS codes and prices through our Data Maintenance Services. These services allow your hospital to easily maintain ongoing updates to your change master through remote access.
ParaRev also offers a full spectrum of healthcare revenue cycle management services, from front-end charge master analysis and contract management, to end-of-cycle zero-balance denial recovery. We’re committed to working seamlessly with your hospital financial and billing staff to minimize denials and bad debt, improve collections, and boost revenues.
Barbara Johnson, BSN, RN, CPC, FHFMA Senior Revenue Cycle Consultant
The No Surprises Act (NSA) is a federal law which went into effect on January 1, 2022. The law bans surprise medical bills for emergency services and elective care when the patient does not have a choice of ancillary service providers in an in-network facility.
The Department of Health and Human Services (HHS) has realized that not all aspects of the NSA will be able to be implemented by providers and facilities by January 1, 2022, so they have elected to exercise “enforcement discretion” on portions of the act in 2022. To be in compliance in 2022, healthcare providers and health care facilities must be prepared to:
Publicize and disseminate a “Disclosure Notice” which informs beneficiaries of group health plans of their rights under the No Surprises Act; and
Publicize and disseminate a “Right to Receive a Good Faith Estimate” to uninsured or self-pay patients; and
Provide uninsured or self-pay patients with a good faith estimate (within a $400 threshold) of services that will be billed by the “convening” provider or facility.
Present a Notice and Consent form, with an estimate of charges, to a beneficiary of a group health plan who chooses to receive services from an out-of-network facility or provider and submit a claim to the health plan.
Disclosure Notice
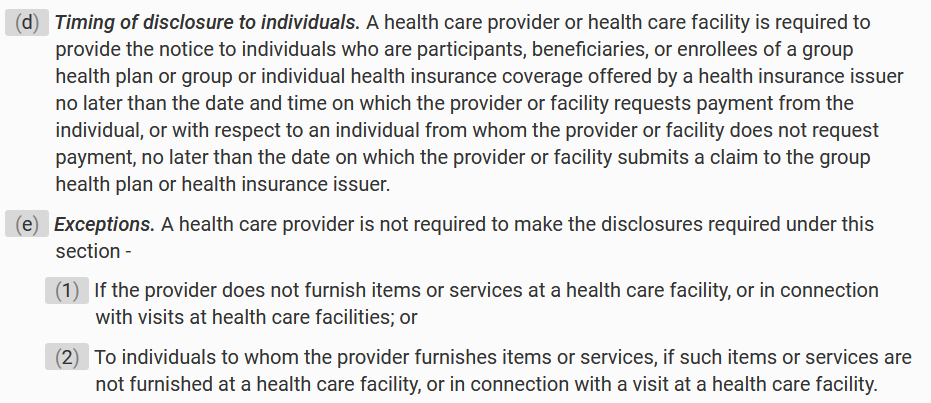
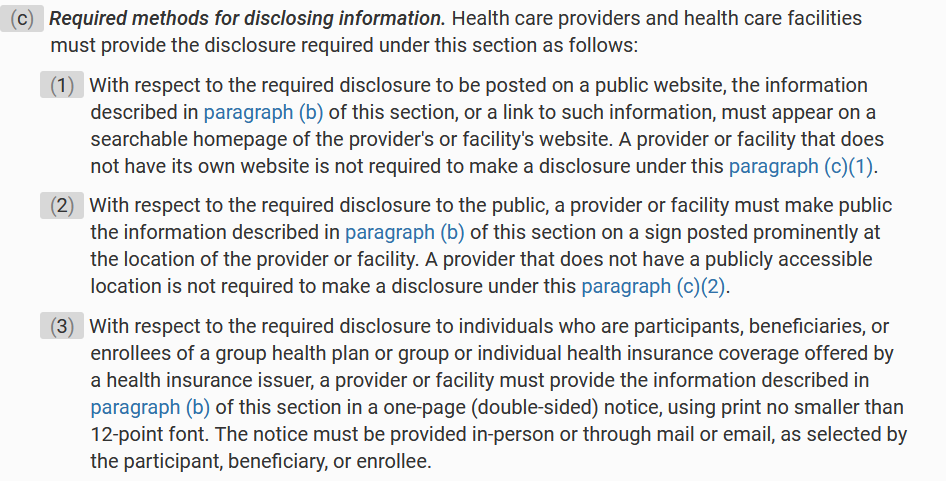
As of January 1, 2022, the disclosure notice must be prominently displayed on websites, in public areas of an office or facility, and on a one-page (double-sided) notice provided in-person or through mail or e-mail, as chosen by the patient. The disclosure notice must be provided to all commercially insured patients after January 1, 2022, or before that date if the elective service will be provided after January 1, 2022. The notice must be provided before requesting a payment from the insured or before a claim is submitted on behalf insured.
In states where there are state laws that protect patients against surprise billing, providers and facilities can use a state disclosure notice if it meets or exceeds the federal guidelines. If a provider or facility drafts their own disclosure notice it must include these three points:
Restrictions on providers and facilities regarding balance billing in certain circumstances
Any applicable state laws protecting against balance billing
Contact information for appropriate state and federal agencies if the individual believes their rights have been violated
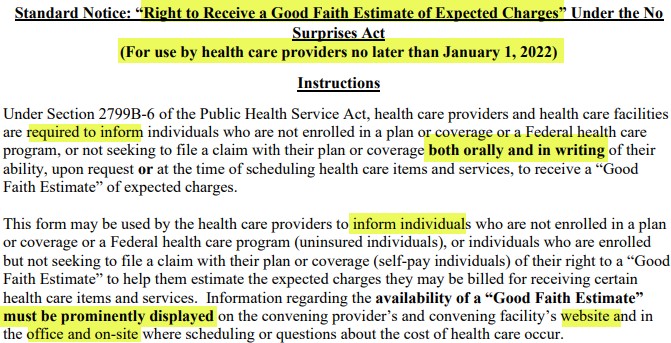
Right to Receive a Good Faith Estimate Notice
All uninsured or self-pay individuals must be made aware, both orally and in writing, of their right to receive a good faith estimate for any services that will be rendered beginning January 1, 2022. The form must be prominently displayed on websites, in offices, and where scheduling or questions about the cost of health care may occur.
Good Faith Estimates to Uninsured/Self Pay
When discussing the good faith estimate it is important to know a few terms:
A health care provider (provider) is defined as a physician or other health care provider who is acting within the scope of practice of that provider’s license or certification under applicable State law.
A health care facility (facility) is defined as a hospital or hospital outpatient department, critical access hospital, ambulatory surgical center, rural health center, federally qualified health center, laboratory, or imaging center that is licensed as an institution pursuant to State laws or is approved by the agency of such State or locality responsible for licensing such institution as meeting the standards established for such licensing.
The convening provider or facility is the one who receives the initial request for a good faith estimate from an uninsured or self-pay individual and who is or, in the case of a request, would be responsible for scheduling the primary item or service.
A co-provider or co-facility furnishes items or services that are customarily provided in conjunction with the convening provider.
An uninsured patient is an individual who does not have benefits for an item or service under a group health plan; whereas a self-pay patient is an individual who has benefits under a group health plan but chooses not to have a claim submitted to their plan. The good faith estimate presented to an uninsured or self-pay patient must include services reasonably expected to be provided by the convening provider or facility. At this time, estimates for services provided by co-providers and co-facilities do not have to be provided by the convening provider or facility.
The following list was provided in the interim final rule published in the Code of Federal Regulations. CMS followed up with a Fact Sheet that clarifies HHS will not be enforcing the requirement of including services provided by co-providers or co-facilities.
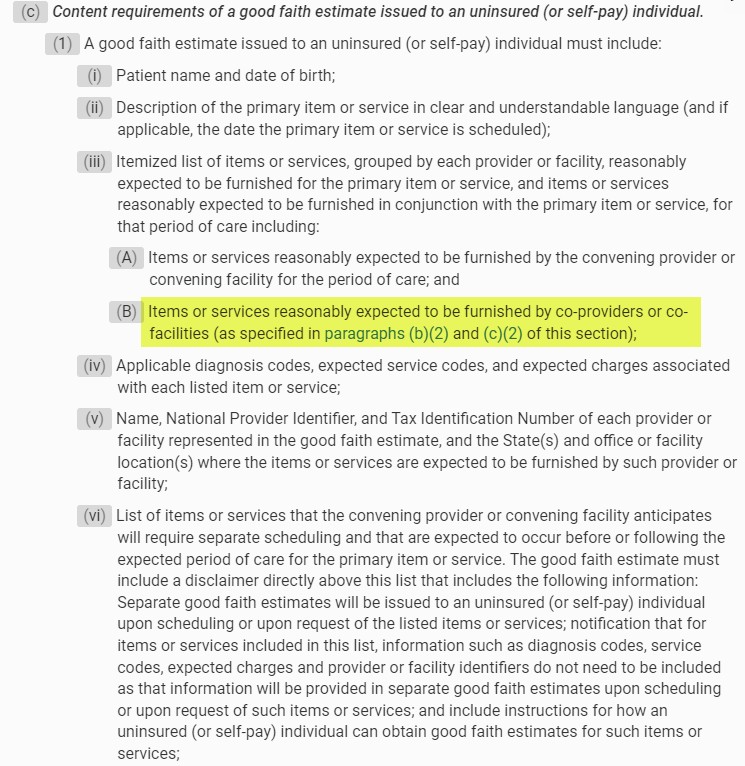
A good faith estimate must include:
Patient name and date of birth
Description of the primary item or service
Itemized list of items or services reasonably expected to be furnished
Items or services reasonably expected to be furnished by the convening provider or convening facility for the period of care; and
Items or services reasonably expected to be furnished by co-providers or co-facilities
Applicable diagnosis codes, expected service codes, and expected charges associated with each listed item or service
Name, National Provider Identifier, and Tax Identification Number of each provider or facility represented in the good faith estimate, and the State(s) and office or facility location(s) where the items or services are expected to be furnished by such provider or facility
List of items or services that the convening provider or convening facility anticipates will require separate scheduling
The Good Faith Estimate process that requires facilities and providers to transmit estimates to health plans, is still on hold.
Notice and Consent
The Notice and Consent is being enforced for those rare instances when the patient has a choice of providers and chooses to receive services from an out-of-network facility or provider. Situations when a patient does not have a choice of providers and cannot be requested to sign a consent waiving their balance billing protections in an in-network facility are:
When receiving services that are considered ancillary services:
Items and services related to emergency medicine, anesthesiology, pathology, radiology, and neonatology
Items and services provided by assistant surgeons, hospitalists, and intensivists
diagnostic services, including radiology and laboratory services
Items and services provided by a nonparticipating provider if there is no participating provider who can furnish such item or service at such facility
Balance billing is prohibited in all emergency situations, even those that arise during a service that is being provided under a written consent. Any charges related to that emergency cannot be balance billed until the patient is deemed stable, as defined in the NSA – able to transport to another facility by nonmedical transportation. In the event the patient requires a higher level of care that requires transport, the EMTALA guidelines take precedence.
A patient admitted to an out-of-network facility from an emergency department who is then considered stable, must be presented with a notice and consent if they choose to continue treatment in the out-of- network facility. If the consent is signed, the out-of-network facility can balance bill for charges incurred after the provider documents that patient is stable, as defined in the NSA – able to transport to another facility by nonmedical transportation. Ancillary services cannot balance bill even after the patient is considered stable.
The Notice and Consent form, with an estimate of all charges, must be presented to the patient for a signature.
This form must be available in the 15 most common languages in the geographical area. If the individual’s preferred language is not among those 15, a qualified interpreter must be made available to assist the patient with understanding their rights.
The form must be provided at least 72 hours prior to scheduled services, when they are scheduled at least 72 hours out. When services are scheduled and performed on the same day, the document is required to be presented at least 3 hours before the services are rendered.
The patient must be provided with a signed copy and a signed copy must be maintained in the medical record in the same manner as all other required documented.
ParaRev can Help
ParaRev has an online tool that can assist with estimates and notices. To learn more, contact us at 800-999-3332 and ask to speak with an Account Executive for more information.
ParaRev offers a full spectrum of healthcare revenue cycle management services, from front-end charge master analysis and contract management to end-of-cycle zero-balance denial recovery. We’re committed to working seamlessly with hospital financial and billing staff to minimize denials and bad debt, improve collections and boost revenues.
ParaRev’s comprehensive capabilities, when aligned with hospital internal teams, can help hospitals improve operating margins and collect additional revenue. Contact us to learn how we can help your facility meet the requirements of the No Surprises Act.
Revenue Cycle Executive Game Plan: Proven Automation Strategies that Deliver Results
Download our free whitepaper to learn how a 6-step end-to-end action plan can transform your revenue cycle operations.
Barbara Johnson, BSN, RN, CPC, FHFMA Senior Revenue Cycle Consultant
In 2019, the Centers for Medicare & Medicaid Services (CMS) announced that calendar year 2020 would serve as a “test and educate” period during which providers billing for advanced imaging studies are required to report whether the ordering physician consulted a clinical decision support mechanism. The requirement to report the informational codes is currently in effect, but Medicare will not yet impose penalties for failure to report, or for incorrect reporting. (The requirement does not apply to Critical Access Hospitals). The Appropriate Use Compliance (AUC) program was authorized by the Protecting Access to Medicare Act of 2014 (PAMA) to promote the use of AUC and decrease the number of inappropriate advanced diagnostic imaging services provided to Medicare beneficiaries.
Ordering physicians (or clinical staff acting at the physician’s direction) will consult the AUC using a clinical decision support mechanism (CDSM). The CDSM is an interactive, electronic tool that is either stand-alone or integrated into an electronic health record (EHR). When queried, it provides a response indicating that the advanced diagnostic imaging service is appropriate, not appropriate, or not applicable for the patient. The AUC requirements apply to advanced diagnostic imaging services (CT, PET, MRI, and Nuclear Medicine) provided in physician offices, hospital outpatient departments (including emergency departments), ambulatory surgical centers, and independent diagnostic testing facilities.
Consulting CDSMs exceptions
CMS released an MLN Matters article in July 2019 that includes the imaging HCPCS codes, the G-codes for the CDSMs, and AUC modifiers. There are a few exceptions to the requirement to consult the CDSM, which are:
Emergencies
Inpatient advanced diagnostic imaging services
Ordering physician meets hardship exception
Hardship exceptions include:
Insufficient internet access
EHR or CDSM vendor issues
Extreme and uncontrollable circumstances
If an exception exists, the physician will include it with the order and the furnishing physician will report the corresponding modifier on the claim.
AUC Requirements
After the physician has consulted the CDSM and ordered the advanced diagnostic imaging service, the following data will be sent, with the order, to the provider completing the imaging service:
The CDSM consulted by the ordering physician.
Whether the service adhered to the applicable AUC, did not adhere to the applicable AUC, or whether no criteria in the CDSM were applicable to the patient’s clinical scenario.
eviCore healthcare’s Clinical Decision Support Mechanism
G1001
MedCurrent OrderWiseTM
G1002
Medicalis Clinical Decision Support Mechanism
G1003
National Decision Support Company CareSelectTM*
G1004
AIM Specialty Health ProviderPortal®*
G1007
Cranberry Peak exCDS
G1008
Sage Health Management Soluntions Inc RadWise®
G1009
Stanson Health’s Stanson CDS
G1010
Radrite*
G1011
AgileMD’s Clinical Decision Support Mechanism
G1012
EvidenceCare’s Imaging Advisor
G1013
InveniQA’s Semantic Answers in MedicineTM
G1014
Reliant Medical Group SCSM
G1015
Speed of Care CDSM
G1016
HealthHelp’s Clinical Decision Support Mechanism
G1017
INFINX CDSM
G1018
LogicNets AUC Solution
G1019
Curbside Clinical Augmented Workflow
G1020
E*HealthLine Clinical Decision Support Mechanism
G1021
Intermountain Clinical Decision Support Mechanism
G1022
Persivia Clinical Decision Support
G1023
New Advanced Diagnostic Imaging HCPCS Modifiers
Medicare also released eight new modifiers to be appended to the imaging HCPCS when an advanced diagnostic imaging is billed. The modifiers indicate the clinician’s use (or non-use) and compliance with a CDSM when ordering advanced diagnostic images.
Modifiers to be appended to Advanced Diagnostic Imaging HCPCS on Medicare Outpatient Claims
Modifier
Short Descriptor
Long Descriptor
MA
Emer med cond susp/confirm
Ordering professional is not required to consult a clinical decision support mechanism due to service being rendered to a patient with a suspected or confirmed emergency medical condition
MB
AUC hardship, insuf internet
Ordering professional is not required to consult a clinical decision support mechanism due to the significant hardship exception of insufficient internet access
MC
AUC hardship, vendor issues
Ordering professional is not required to consult a clinical decision support mechanism due to the significant hardship exception of electronic health record or clinical decision support mechanism vendor issues
MD
AUC hardship, extreme circ
Ordering professional is not required to consult a clinical decision support mechanism due to the significant hardship exception of extreme and uncomfortable circumstances
ME
Order adheres to AUC
The order for this service adheres to the appropriate use criteria in the clinical decision support mechanism consulted by the ordering professional
MF
Order does not adhere to AUC
The order for this service does not adhere to the appropriate use criteria in the clinical decision support mechanism consulted by the ordering professional
MG
AUC not applicable to order
The order for this service does not have applicable appropriate use criteria in the qualified clinical decision support mechanism consulted by the ordering professional
MH
AUC consult not provided
Unknown if ordering professional consulted a clinical decision support mechanism for this service, related information was not provided to the furnishing professional or provider
The excerpt below illustrates the mandatory reporting for a CT of the head billed to Medicare on a UB04:
AUC workflow requirements
The following is the workflow for meeting the AUC requirements:
The physician sees a Medicare beneficiary and plans to order an advanced diagnostic imaging service
The physician (or clinical staff under the direction of the physician) consults the AUC for the proposed advanced diagnostic imaging service through a CDSM. The CDSM can be integrated into the EHR or a separate portal
If a hardship exception exists, the physician will include it with the order
The CDSM will search for and present the AUC relevant to the patient’s condition
The CDSM response will indicate if the proposed advanced diagnostic imaging service:
adheres to the AUC, or
does not adhere to the AUC, or
if there is no applicable AUC
If it adheres to the AUC, the physician will proceed with the order
If it does not adhere, the physician must decide to order a different imaging service or proceed with the proposed service despite it not adhering to the AUC
The physician orders the advanced diagnostic imaging service and includes with the order:
the CDSM queried, and
the AUC response, and
the physician’s NPI
The rendering provider furnishes the imaging service to the patient
The rendering provider reports in the professional and institutional claims:
HCPCSG-code associated with the CDSM, and
The applicable AUC modifier, and
the ordering physician’s NPI
Analysis of ordering physician practices
The outcome of this program will be to analyze the ordering practices of the physicians and determine any outliers. PAMA calls for identification on an annual basis of no more than five percent of the total number of ordering physicians who are outliers. The use of two years of data is required for this analysis. Data collected during the education and testing period will not be used when identifying outliers. Outliers will be determined based on low adherence to applicable AUC or comparison to other ordering physicians. Physicians who are found to be outliers will be required to complete prior authorizations for advanced diagnostic imaging services.
The following clinical areas will be the focus of the analysis of outliers:
Coronary artery disease (suspected or diagnosed)
Suspected pulmonary embolism
Headache (traumatic and non-traumatic)
Hip pain
Low back pain
Shoulder pain (to include suspected rotator cuff injury)
Cancer of the lung (primary or metastatic, suspected or diagnosed)
Cervical or neck pain
Compliance Assistance
Pararev can provide compliance assistance to help you navigate the Appropriate Use Criteria (AUC) for Advanced Diagnostic Imaging regulation.
Pararev is a revenue cycle solutions provider that offers price transparency, reimbursement, revenue integrity/coding, and compliance support. Comprised of seasoned professionals and equipped with a web-based cloud computing engine, the Pararev Data Editor (PDE), they analyze, identify, repair, and improve the revenue cycle processes to support Providers in achieving their financial goals.
Pararev is comprised of a team of coders, compliance experts, financial analysts, and IT professionals with extensive experience in focused disciplines to support the revenue cycle process. In fact, on average, our consultants have over 21 years of healthcare experience, allowing them to support clients with experience from the trenches. Pararev’s services range from a web-based revenue cycle tool to a comprehensive revenue integrity program complete with a chargemaster audit, pricing services, monthly department meetings, and ongoing pricing, coding, reimbursement, and compliance support.
Contact us to learn more about how we can help you navigate today’s healthcare compliance concerns including the Appropriate Use Criteria (AUC) for Advanced Diagnostic Imaging regulation and more.
Zero-balance claims reviews represent a final safety net that can generate hundreds of millions of dollars for hospitals